

What is Physician Coaching and How Does it Compare to Faculty Coaching-Skills?
This post is part of the Faculty Coaching Skills Series, which explores how faculty can apply coaching approaches in medical education.
When you read the literature around physician coaching in graduate medical education (GME), you will notice the word “coaching” is used in different contexts to convey different connotations. I want to conclude this blog series by comparing and contrasting (and seeing the overlap between) physician coaching and the use of coaching skills by faculty.
I was working on a Physician Coaching White Paper (coming soon) within the CHARM (Collaboration for Healing and Renewal in Medicine) Coaches group when I was asked to consider presenting for the Society of Teachers in Family Medicine (STFM) in a webinar series for Faculty Development on Competency-Based Medical Education about coaching - Advisors and Coaches: The Evolving Role of Faculty. It was perfect timing as we had been wrestling with the terminology published in the literature for the white paper. It had become clear that the term “coaching” in academic medicine was used variably, and there needed to be some standardization around definitions.
For background, undergraduate medical education (UME) adopted coaching more broadly earlier than GME, following the AMA’s Faculty and Student Guidebooks on Coaching. They have proactively recorded basic coaching videos , and many medical schools host training for UME faculty (that can be useful for GME faculty as well). Excitingly, in mid-2024, the AMA published its Coaching in Graduate Medical Education: A Faculty Guidebook. Cleveland Clinic and Mass General, and I suspect many other universities, offer basic coach skills training for faculty (see my previous blog on training).
Let’s start with what the literature reveals about coaching in medicine and GME. It supports:
- Technical skills (e.g. procedures)
- Non-technical skills (e.g interpersonal)
- Cognitive skills (e.g. developing a differential diagnosis)
- Well-being (e.g. flourishing, enganged - more than the absence of burnout)
- Other various professional development (e.g. personal identity formation, leadership, etc)
At the core of all of these lies 3 key building blocks
- Growth Mindset and Appreciative Inquiry - in which any failure or mistake is seen as growth opportunities and the negativity bias is balanced by focusing on what is going well, in order to build self-efficacy.
- Metacognition – thinking about one’s own thoughts.
- Unconditional positive regard by the coach toward the coachee.
Other commonalities include
- Dialog - coaching conversations in which the coachee is generating new insights, perspectives, and clarity.
- Initiative and Ownership - the coachee is taking ownership of moving forward.
- Growth - they all enhance one's development (personally and/or professionally)
However, what the term “coaching” means beyond that in the literature varies. I’m offering you my favorite way of understanding two categories put forth by Elaine E. SchulteMD, MPH, PCC, BCC, though, there are other ways to slice and dice it out there. Just like I can julienne some potatoes and call them fries or slice it and call it scalloped potatoes – there are other categorizations that differ from below – and that’s okay as the literature is exploding while everyone is tackling the best way to understand and explain it all.
- Most of the literature for the technical, non-technical, and cognitive skills takes a performance-based approach (skill-based coaching).
- Most of the well-being and professional development literature highlights developmental coaching (what the coaching profession simply calls professional coaching or coaching).
Performance Based, or Skills-Based Coaching, in GME is more akin to the sports or performing arts coach analogy. It’s essentially the coaching approach to the Clinical Educator Hat. Whether involving procedures, communication skills, or developing differential diagnosis, there is a shared ownership of the growth process – an alliance if you will. The faculty use their expertise, while the learner can be the source of ideas. It often (but not always) involves observation and feedback (specifically the coach’s feedback). Many of the formalized feedback and precepting tools are coach-approach frameworks (e.g. Prepare to ADAPT, R2C2, Ask-Tell-Ask, etc.).
Developmental Coaching is formal Physician Coaching (or as professional coaches, what we mean simply by the term, Coaching). Some faculty may actually be trained and wear a formal Coaching Hat (or the program may use an external coach). This does not rely on observation or feedback, and if any is incorporated into the conversation, it explicitly does not include the faculty-coach’s feedback because the coach in this context is neutral. The expertise and source of ideas both lie within the learner-coachee.
I want to camp out a bit on the role of faculty applying coaching skills.
I find it best to visualize various approaches of interacting with residents on a spectrum.
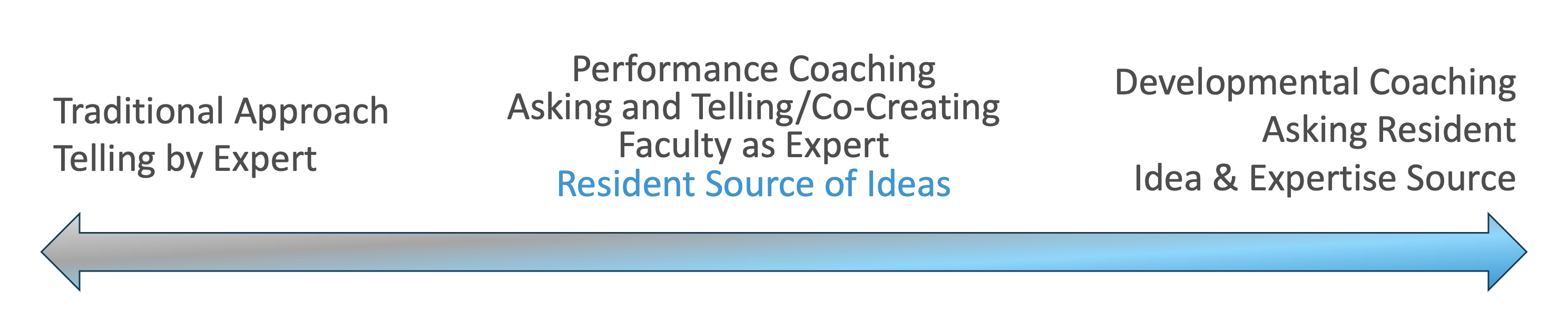
Sometimes, as the faculty, you will need to take a more directive (telling) approach as the expert, while at other times, it will be more useful to take that performance- skills-based coaching approach.(More on this in a minute*) And a few of you, may be trained and have a formal coaching role with residents in that developmental coaching manner.
Most of our daily work, though, happens in what I call the Co-Creation Zone, the middle that’s actually more of a spectrum, where faculty and learners share both expertise, ideas and reflection. Coaching in this space helps residents take greater ownership of their learning, internalize the lessons better, while still benefiting from your clinical guidance. Even if pure developmental coaching sits more in the domain of formally trained coaches, you can begin to stretch toward that side of the spectrum by learning to pause and draw out their own expertise before inserting yours. Sometimes the greatest teaching moment comes from staying curious long enough for them to find their own reasoning, and then helping them refine it rather than replace it.
Consider our faculty roles in light of being Master Adaptive Learners (MAL) who are invested in having our trainees become MAL themselves. This is such a crucial development in order to weather the unknown and unending changes ahead in GME and medicine – whether it be health policy changes, rapidly expanding clinical information and data, new pandemics, limited resources, etc – coaching is crucial to develop into MAL. Wolff M. et al. Instilling the ability to grow in self-assessment, metacognition, self-reflection, and self-direction is a natural outcome of participating in coaching.
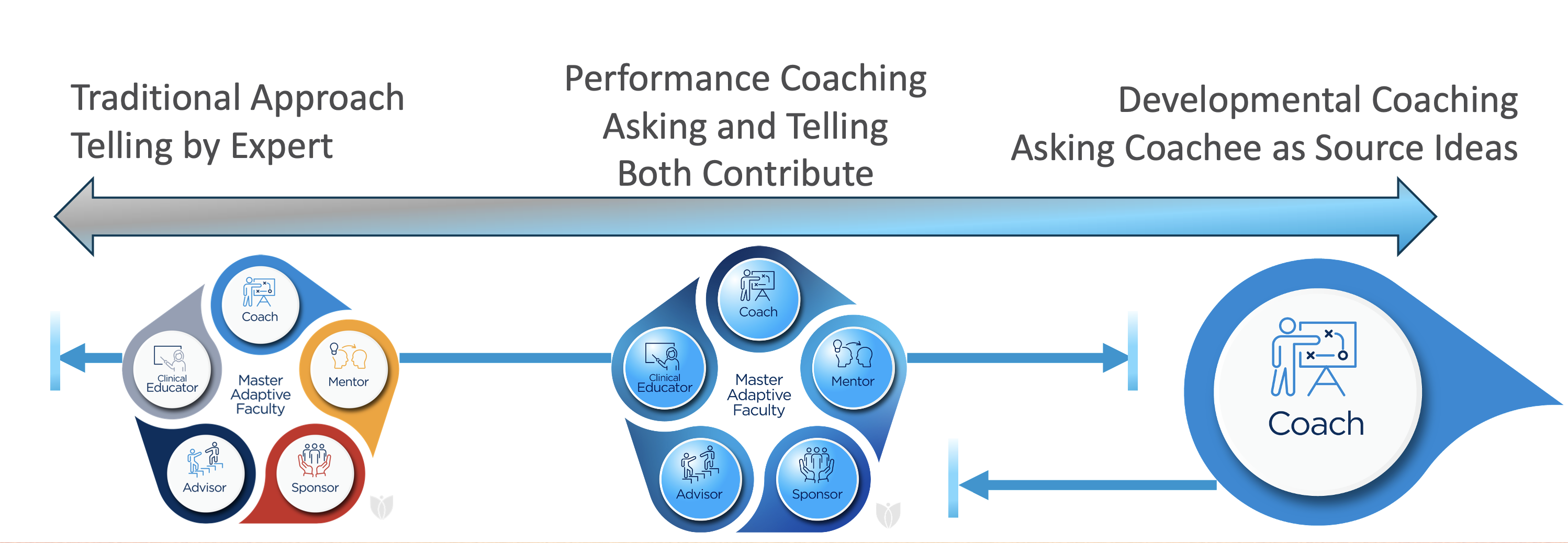
As MAL’s in your faculty role, Master Adaptive Faculty, you potentially wear 5 different hats as you relate to your residents and fellows. (most of the language* below credited to Dr. Tony Tsai University of Utah).
Clinical Educator Hat (teaching, supervising, evaluating), imparting knowledge and skills
Advisor Hat, imparting information from your expertise*
Mentor Hat, imparting perspective from your experience*
Sponsor Hat, imparting connection to opportunities via endorsement*
Formal Coach Hat, facilitating clarity and confidence*

In the business sector, executives and middle managers have been taught coaching skills for decades. But, they don’t go out and become certified coaches, they learn basic skills and take a coaching-approach when appropriate in their current roles because it is often much more impactful.
So, if we were to imagine putting on the blue lenses of coaching and viewing faculty roles through them, we can see that we can perform those roles with a more coach-approach. And, then learn when to take the performance/skill-based coaching approach and when to take the telling-by-expert approach.

This is where you need your own learner's mind and growth mindset. Understanding that over time, with practice, you will learn in which situations, with which individuals one lens/approach serves better than the other. (For more on seeing it as a growth mindset in your roles - remember coaching is one of the universal pillars in the Faculty Development Milestones from the Clinical Educator Milestone Project). Graphically, I illustrate that here:
As you approach a trainee (or are approached), it’s helpful to consider which approach is best in that moment.
By way of analogy, when you go to the optometrist, you have to decide if Lens 1 (telling) or Lens 2 (asking, clarifying, discussing, asking) is best.
If you have the answer, it doesn't seem kind to try to get them to tell you what you are thinking, so you pick Lens 1 (exceptions would be employing the Socratic method properly—which is very misunderstood). Trying to lead someone to the answer you feel is best is not coaching.
For example: They want to know which med is most effective in A Fib with RVR in the patient admitted with it or how to set up an away rotation. There is usually the answer you have and they need that information imparted to learn.
If you can see the trainee as whole, capable, and resourceful and be humble enough to believe you don’t have their best answer for a particular situation, then a coaching approach, Lens 2, is very useful. In some situations, it may seem more clear to use coaching skills rather than telling them your opinion.
For example: They can’t decide when they want to have children given their age and still being in training and bring the subject up to you.
Other times, just like the optometrist, both lenses may look the same. You just have to pick one and see what you learn.
For example: They want to talk to you because they’re feeling guilty about wanting to run a direct primary care practice rather than work at an FQHC. Lens 1 - Telling your perspective as their mentor based on your experience or Lens 2 Taking a coaching approach and asking questions to help them gain clarity - both seem good.
Coaching as faculty, involves you growing your skills and choosing when to use them. Putting it visually a slightly different way thinking of the most common situations you as faculty will employ coaching: 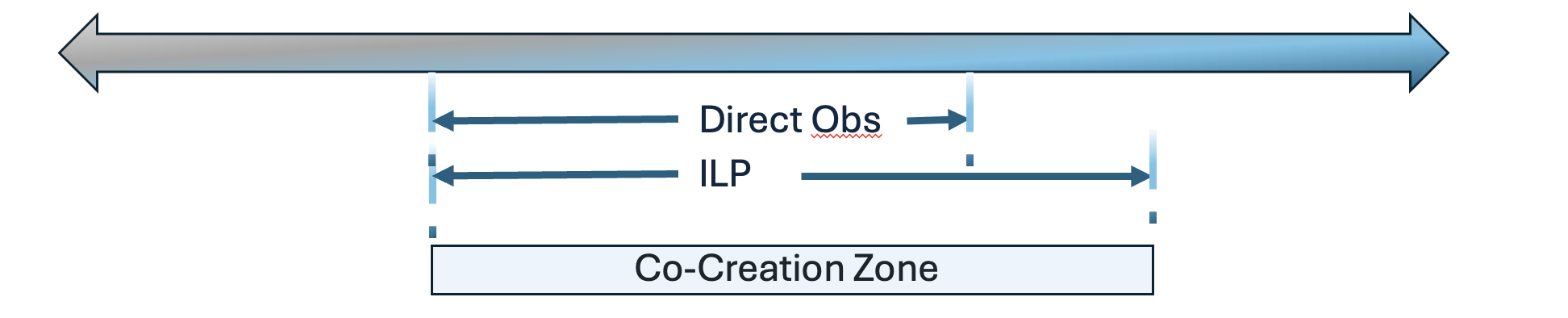
*But what does it look like for a faculty member to take a coaching approach? Again, it’s a conversation in which you use questions to help further the thinking and insights of the trainee. And, you also inform them based on your expertise and opinion from experience. Here's an example:
Resident: I’m wanting to work on becoming more efficient in the room with patients.
Faculty: Great, I’d like to take a coaching approach with you in order to facilitate an answer that will be most useful, is that okay?
Resident: Yes.
Faculty: What’s the reason you’re wanting to be more efficient?
Resident: So I can leave on time, not make people wait on me, and not have a ton left to do after work hours.
Faculty: I see, what’s the biggest barrier for you?
Resident: Limiting the amount of things I do in the room.
Faculty: What’s the hardest part of that for you?
Resident: So many of our patients have a hard time getting here, and it’ll be awhile before I can get them back in.
Faculty: So it sounds like you’re a caring family doctor who wants to help their patients.
Resident: Yes.
Faculty: Can I offer a suggestion?
Resident: Yes.
Faculty: We know from studies on Relationship-Centered communication, patients appreciate being able to let us know what they want to cover and take part in the decision making of what we cover in today’s visit. If you knew your patient was actually going to appreciate the agenda setting process, what would change for you?
Resident: I guess, I would feel a little less guilty not getting to everything.
Faculty: Great, what’s one thing you can try today in clinic in regards to that?
Resident: I guess, working on how I agenda set. What do you say?
Faculty: Well, I’ve tried various things over the years and what feels good to me is to say, “I wish I had unlimited time to cover everything important to you in this 20 minute visit. However, I don’t have that luxury. If we can only get to one or two things today on what you listed for the medical assistant, what would you say are the most important? Great. Let’s cover those and if you don’t mind, I really think we need to address your anemia, how does that sound?"
Resident: Okay, well I can modify that to sound more like me and try it out.
Both contribute, the resident is seen as having a good source of ideas and needing to think through what the barriers are and inquiry is used to elicit them; the faculty share their expertise: there is a back and forth in co-creating the next steps.
Okay, we have one more blog (maybe two 😉) in this series, next week, I’ll touch on individualized learning plans, ILP, and attempt to highlight the challenging areas for faculty to change to the coaching-lens along with some tips.
Until then,
Have a joy-filled week! Tonya
If you're looking for some faculty development around coaching or an external coach, reach out.
Join Weekend Reads
Weekly insights, tips, and tools for physicians who want to thrive—plus a dash of fun.
We hate SPAM. We will never sell your information, for any reason.
